

Abstract
Introduction
Ixazomib is an effective PI that combines the advantage of oral administration with a favorable toxicity profile. Recent results showed significant activity, both in newly diagnosed, and in pretreated patients (pts). Ixazomib in combination with lenalidomide-dexamethasone (IRd) was significantly superior over Rd in pts with relapsed/refractory multiple myeloma (RRMM), and was able to overcome the negative impact of poor risk cytogenetics. Ixazomib-thalidomide-dexamethasone (IxaThalDex) has been shown to be effective in pts with newly diagnosed MM and is used in this trial in pts with RRMM. Here, we evaluate the impact of cytogenetic risk factors on outcome in pts with RRMM treated with IxaThalDex.
Patients and Methods
Ninety pts with RRMM and one or more prior lines of therapy (TX) were enrolled. Treatment regimen: Ixazomib (4mg, d 1, 8 and 15), thalidomide (100mg/d), and dexamethasone (40mg once/week). Pts aged ≥75 years received lower doses of thalidomide (50mg/d) and of dexamethasone (20mg). Pts were scheduled for 8 cycles followed by ixazomib maintenance therapy (4mg, days 1, 8, 15 of a 28 cycle and 3mg in pts aged ≥75 years) for one year. Preplanned FISH analysis was performed on CD138 selected bone marrow plasma cells. The cut-off level for positivity was 10% for t(4;14), and 20% for del(17p) and 1q21 gain, respectively. The previously defined primary endpoint was progression-free survival (PFS), and secondary objectives were overall response rate, overall survival (OS), and impact of cytogenetic risk and of renal impairment, safety and myeloma frailty status. PFS and OS was estimated according to Kaplan-Meier and differences evaluated by log-rank test. Response rates were compared using Fisher's Exact Test.
Findings
Seventy-six of the 90 pts of the intent to treat group (ITT) received at least two cycles and comprise the per protocol population (PP). Complete FISH data are available in 61 pts. Pt characteristics of the ITT group: Age, median 67 (44 -84) years, ISS stage I: 37, II 30, III: 22, not known: 1, median number of prior TX lines: 1 (range: 1-8). Forty-three pts have completed all 8 cycles of induction therapy (median number of cycles: 6). Forty-one pts started Ixazomib maintenance therapy and 6 completed the planned 12 cycles as yet.
Median follow-up is 15.3 months. PR or better was achieved in 46 pts (60.5%), CR in 8 (10.5%), VGPR in 13 (17.1%), PR in 25 (32.9%), and MR in 6 (7.9%) pts, yielding a clinical benefit rate of 68.4%.
Thirteen (21.3%) pts of the 61 pts with FISH data available presented with t(4;14), 5 (8.1%) with del(17p), and 32 (52.5%) with 1q21 gain. Response rates (≥PR) did not differ significantly (p values not shown) between pts with high-risk (HR) [t(4;14) and/or del(17p)], and standard-risk (SR) cytogenetic risk profile: 64.7% vs. 53.2%, nor in those with and without 1q21 gain: 46.9% vs. 69.2%, or those with HR cytogenetics and/or 1q21 gain 48.7% vs. 68.2, and were comparable to those of the entire PP patient group (60.5%).
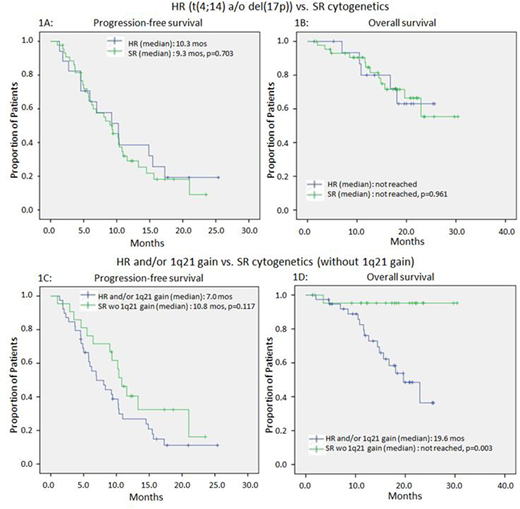
Median PFS at the time of reporting is 8.8 mos. in the ITT and 10.2 mos. in the PP group. PFS did not differ in pts with HR and SR cytogenetics (10.3 vs. 9.3 months, p=0.703). In contrast, a tendency for shorter PFS was noted in pts with 1q21 gain (6.9 vs. 11.6 months, p=0.067). Similar findings were observed in pts with HR and/or 1q21 gain vs. those without these features (7.0 vs. 10.8 months; p=0.117).
Median OS has not been reached, neither in the ITT nor in the PP group. OS did not differ between pts with HR and SR cytogenetics (p=0.961), similarly, Pts with 1q21 gain had significantly shorter OS (median: 19.6 vs. not reached, p=0.001); a similar reduction in OS was noted when pts with HR cytogenetics and/or 1q21 gain were compared to those without these features (median: 19.6 months vs. not reached, p=0.003)
Discussion and Conclusion
The all oral IxaThalDex regimen overcame the negative impact of HR cytogenetics [t(4;14) and del(17p)] both in terms of PFS and OS. Similarly, there was no difference in the depth of response between the groups. However, in those with 1q21 gain alone, or with a HR feature and/or 1q21 gain, a tendency of shorter PFS was noted. OS was significantly shorter in the latter groups. These findings suggest that 1q21 gain should be included in the HR category in pts exposed to ixazomib plus thalidomide-dexamethasone.
Figure 1: PFS and OS in pts with and without HR cytogenetics (1A and 1B) and in those with and without HR cytogenetics and/or 1q21 gain (1C and 1D).
Ludwig:BMS: Speakers Bureau; Takeda: Research Funding, Speakers Bureau; Celgene: Speakers Bureau; Amgen: Research Funding, Speakers Bureau; Cilag-Janssen: Speakers Bureau. Knop:Bristol Myers Squibb: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding. Hajek:Amgen: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding; Bristol-Myers Squibb: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding. Gunsilius:Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen-Cilag: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; BMS: Honoraria. Petzer:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees. Weisel:Amgen, Celgene, Janssen, and Sanofi: Research Funding; Amgen, BMS, Celgene, Janssen, Juno, Sanofi, and Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen, BMS, Celgene, Janssen, and Takeda: Honoraria. Greil:Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Astra Zeneca: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; MSD: Honoraria, Research Funding; Sandoz: Honoraria, Research Funding; BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Honoraria, Other: TRAVEL, ACCOMMODATIONS, EXPENSES, Research Funding; Merck: Honoraria, Research Funding; Janssen: Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees.

